HomeBlogs
Stem Cell Therapy Combined with Therapeutic Apheresis for Type 1 Diabetes
Stem Cell Therapy Combined with Therapeutic Apheresis for Type 1 Diabetes
Type 1 diabetes is one of the most demanding conditions a person can live with. While daily management is challenging, the greater problem is the underlying cause: the immune system attacking insulin-producing cells, a process standard medicine still cannot repair. Insulin keeps people alive. It does not address why the beta cells stopped working. For patients and families who have spent years managing blood glucose, adjusting doses, and navigating the unpredictability of the condition, the question is not whether current treatment works. It does. The question is whether anything can go deeper, addressing the autoimmune process itself and attempting to restore some of the function lost.
At GS Medical Services in Dubai, we coordinate access to a structured combination therapy programme for selected patients with Type 1 diabetes through specialist clinics in Germany. This programme combines therapeutic apheresis with mesenchymal stem cell (MSC) therapy and targeted immunosuppression. We manage every aspect of the referral, coordination, logistics, and follow-up process, so that patients from the UAE, the Gulf region, and internationally can access this approach with proper clinical support.
Understanding Type 1 Diabetes and the Autoimmune Process
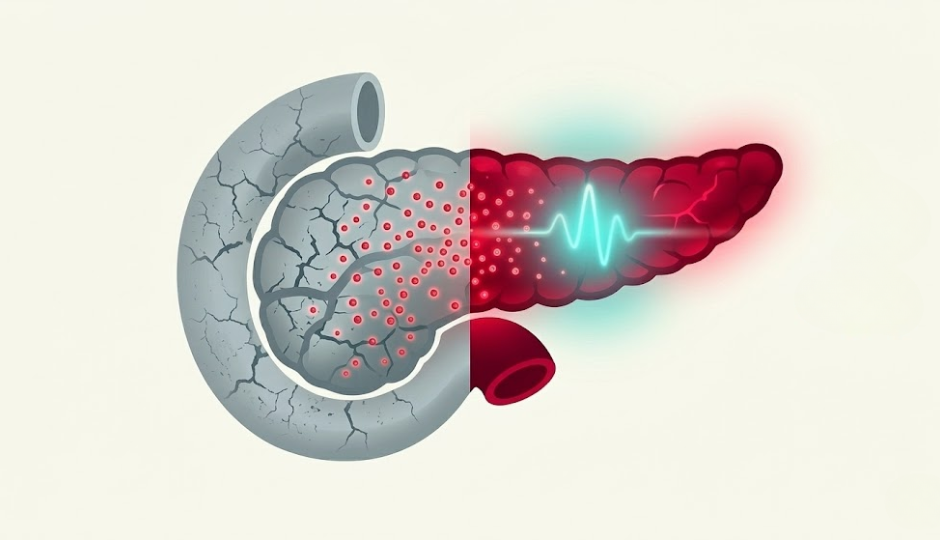
Type 1 diabetes is an autoimmune condition. The immune system, for reasons that are not fully understood, produces antibodies that specifically target and destroy the insulin-producing beta cells of the pancreas. As beta cell mass declines, the body's capacity to produce insulin declines as well, until exogenous insulin, injected or infused, becomes necessary for survival.
Unlike Type 2 diabetes, which involves insulin resistance and a different disease mechanism, Type 1 diabetes is characterised by immune-mediated beta cell destruction. This distinction matters because any meaningful intervention for Type 1 must address the autoimmune process, not simply its metabolic consequences.
Research has identified five key autoantibodies consistently associated with beta-cell destruction in Type 1 diabetes:
Islet cell antibodies (ICA): Among the earliest markers identified, targeting proteins within the islet cells of the pancreas
Glutamic acid decarboxylase antibodies (GADA / anti-GAD65): Present in the majority of Type 1 patients, often detectable years before diagnosis
Insulin autoantibodies (IAA): Particularly common in younger patients at diagnosis
Insulinoma-associated antigen-2 antibodies (IA-2A): Associated with more rapid progression to clinical disease
Zinc transporter 8 antibodies (ZnT8A): One of the more recently characterised markers, found in a substantial proportion of Type 1 patients
These antibodies are not simply bystanders. Their presence at significant titres reflects ongoing autoimmune activity that continues to damage residual beta cell function even after diagnosis. This is why simply replacing insulin does nothing to slow the underlying disease process.
The clinical consequences of Type 1 diabetes include:
Complete or near-complete insulin deficiency, requiring lifelong insulin replacement
High risk of hypoglycaemia (dangerously low blood sugar), which can be life-threatening
Hyperglycaemic episodes, which, over time, contribute to serious complications
Long-term vascular complications, including diabetic nephropathy (kidney disease), retinopathy (eye disease), neuropathy (nerve damage), and cardiovascular disease
Significant daily management burden, affecting quality of life, occupational function, sleep, and mental health
Psychological impact, including diabetes distress and elevated rates of anxiety and depression
Standard Treatment Options for Type 1 Diabetes
Current standard care for Type 1 diabetes centres on insulin replacement and blood glucose monitoring. Advances in technology, such as continuous glucose monitoring (CGM) systems and insulin pumps, have materially improved day-to-day management, but they remain tools for managing the condition. They do not alter the disease. Despite these advances, each approach has important limitations:
Treatment
Limitation
Insulin therapy (injections or pump)
Replaces insulin but does not address autoimmune destruction of beta cells
Continuous glucose monitoring (CGM)
Improves monitoring accuracy but does not treat the condition
Sophisticated management technology does not preserve or restore beta-cell function
Immunotherapy (e.g., teplizumab)
Approved for delay of Stage 3 Type 1 in at-risk individuals; not a cure; limited availability
Islet cell or pancreas transplantation
Reserved for very specific cases; requires lifelong immunosuppression; significant donor shortage
The fundamental problem with all of these approaches is that none of them addresses the ongoing autoimmune process in patients who already have established Type 1 diabetes. The immune system continues attacking whatever residual beta cell function remains. This is the gap that the combination therapy programme is designed to address.
The Combination Therapy Approach: How It Works?
The logic behind combining them is clinical: each component addresses a different part of the problem. Therapeutic apheresis clears the autoantibodies from the system. Mesenchymal stem cell therapy supports beta cell regeneration and immune rebalancing. Immunosuppression maintains the immune reset and protects newly regenerating cells from further attack.
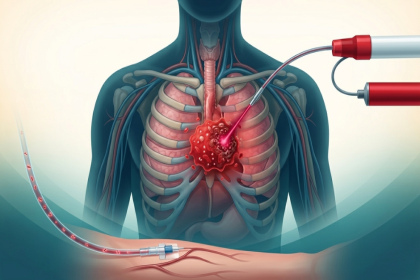
Phase 1: Therapeutic Apheresis; Clearing the Autoimmune Load
The first stage of the programme uses therapeutic apheresis to remove circulating autoantibodies associated with beta-cell destruction from the patient's bloodstream.
Apheresis works by passing the patient's blood through a separation system outside the body, selectively filtering out target components, and returning the treated blood. In the context of Type 1 diabetes, the procedure is used to reduce the burden of the five key autoantibodies (ICA, GADA, IAA, IA-2A, ZnT8A) that are driving ongoing autoimmune damage to the pancreas.
The rationale is straightforward: before attempting to repair or regenerate beta cell function, the immune environment needs to be as clean as possible. Introducing stem cells into a system still loaded with active autoantibodies is less likely to be effective. Apheresis addresses this directly.
Multiple sessions are typically required throughout the treatment programme. The procedure takes place under medical supervision in a clinical setting and is generally well tolerated, though side effects do occur.
Following the apheresis phase, mesenchymal stem cell therapy is administered. MSCs are adult stem cells derived from specific tissue sources and are well characterised in the scientific literature for their immunomodulatory and regenerative properties.
In the context of Type 1 diabetes, MSCs are thought to act through several mechanisms:
Immunomodulation: MSCs can actively suppress aberrant immune responses that drive beta cell destruction. They interact with T-lymphocytes and other immune cells, dampening the autoimmune activity that characterises Type 1 diabetes. This is particularly relevant when the apheresis has cleared the existing antibody load. The MSCs help to rebalance the immune system at a cellular level.
Beta cell support and potential regeneration: MSCs secrete a range of growth factors and signalling molecules that may support the survival of remaining beta cells and, in some patients, stimulate regeneration of new insulin-producing cells. The pancreas retains a degree of regenerative capacity, particularly in patients with some residual beta-cell function.
Anti-inflammatory effect: Chronic low-grade inflammation in the pancreatic tissue contributes to ongoing beta-cell loss. MSCs can reduce this inflammatory environment, creating conditions more conducive to repair.
Paracrine signalling: Rather than directly becoming new beta cells, MSCs appear to work primarily through the factors they secrete, influencing neighbouring cells and the local tissue environment. This paracrine mechanism is now understood to be central to how MSC therapy exerts its effects across a range of conditions.
MSC therapy is administered by qualified physicians at licensed clinics in Germany via intravenous infusion or, depending on the protocol, targeted delivery. The method used is determined during the individual treatment planning process.
Phase 3: Immunosuppression; Protecting the Reset
The third component of the programme is a structured immunosuppression protocol, initiated following stem cell therapy and continued for a defined period thereafter. The purpose of immunosuppression is twofold.
First, it protects newly regenerating or surviving beta cells from being attacked by a recovering immune system before the immune rebalancing achieved by MSC therapy has had time to stabilise.
Second, it supports the durability of the immune reset, reducing the risk of the autoimmune process re-establishing itself.
The specific agents used, dosing, and duration are determined by the treating physician based on the individual patient's profile, disease history, and biological response. Immunosuppression carries its own risk profile, which is discussed comprehensively during your evaluation and monitored carefully throughout the programme.
Important note: This combination approach is not a guaranteed cure for Type 1 diabetes. Outcomes vary considerably between patients and depend on multiple factors, including residual beta cell function at the time of treatment, disease duration, individual immune profile, and adherence to the full programme. GS Medical Services coordinates access to this therapy based on a thorough medical evaluation.
What to Expect During the Treatment Programme in Germany?
Programmes combining stem cell therapy and therapeutic apheresis for Type 1 diabetes are designed to provide personalised, carefully coordinated care. GS Medical supports patients by organising each step of the journey, from initial case review and clinic referral to treatment logistics and follow-up coordination.
Step 1: Comprehensive Medical Review and Eligibility Assessment
Your journey begins with a detailed evaluation to determine whether the combination therapy programme is appropriate for you:
Full clinical history, including diabetes duration, current insulin requirements, HbA1c trends, hypoglycaemia frequency, and complication status
Review of autoantibody titres (ICA, GADA, IAA, IA-2A, ZnT8A) and C-peptide levels; the latter provides an indication of residual beta cell function, which is relevant to treatment candidacy
Assessment of immune function and overall health status
Review of previous diabetes management history and response to treatment
In-depth consultation with the medical team
Honest assessment of whether the combination programme is appropriate, including a frank discussion of expected outcomes based on your individual profile
Step 2: Personalised Treatment Planning
If assessed as a suitable candidate, a fully individualised treatment plan is developed:
Tailored protocol covering the number of apheresis sessions, the MSC therapy approach, and the immunosuppression regimen
Clear explanation of the procedure sequence, timeline, and realistic outcome expectations
Transparent discussion of potential benefits, risks, and alternatives
Comprehensive logistics coordination for international patients, including appointment scheduling, documentation, travel arrangements, and accommodation guidance
Step 3: The Treatment Programme
The full combination programme is conducted at licensed clinics in Germany under qualified physician supervision:
Therapeutic apheresis: Conducted over multiple sessions in a clinical setting, each session lasting several hours. The blood is processed through an apheresis machine to selectively reduce autoantibody levels. Sessions are spaced according to the individual protocol.
MSC therapy: Administered following the apheresis phase via intravenous infusion. On an outpatient basis, patients typically return to their accommodation the same day. Sterile clinical environment with full infection control protocols in place and physician supervision throughout.
Immunosuppression: Initiated following MSC therapy. The treating physician provides clear guidance on the protocol, monitoring requirements, and what to watch for throughout this phase.
The full treatment programme typically lasts days to weeks in Germany, depending on the number of apheresis sessions required. Your schedule is planned in advance, and all clinic appointments are coordinated by our team.
Step 4: Structured Follow-Up and Progress Monitoring
Monitoring after treatment is integral to the programme, not an afterthought:
Remote follow-up via secure telemedicine, removing the need for repeated international travel
Metabolic monitoring, including HbA1c, C-peptide levels, fasting and stimulated insulin measurements, and continuous glucose monitoring data review
Autoantibody retesting at defined intervals to assess the durability of the immune response
Ongoing immunosuppression monitoring as required
Personalised guidance on diabetes management, nutrition, and lifestyle optimisation, alongside the cellular therapy
Direct access to the medical team throughout your recovery and follow-up period
Who May Be a Suitable Candidate?
The combination programme is not appropriate for every patient with Type 1 diabetes. Based on current clinical evidence and the experience of the clinics we coordinate with, candidates most likely to be considered for treatment typically include:
Confirmed Type 1 diabetes with positive autoantibody status (one or more of the five key autoantibodies present at significant titres).
Detectable residual beta cell function, as measured by a measurable C-peptide level, suggests that some beta cell mass remains, which is important for the regenerative component of therapy. Patients with completely absent C-peptide may gain less from this aspect of the programme, though each case is assessed individually.
Duration of diabetes is considered; patients earlier in their disease course may have more residual beta cell function, though patients with longer-standing Type 1 are also assessed, and some may still be suitable.
Suboptimal glycaemic control despite optimised insulin therapy, particularly those experiencing significant hypoglycaemia unawareness or wide glycaemic variability.
Generally stable overall health without significant active infections, malignancy, or other conditions that would complicate treatment or immunosuppression.
No contraindications to therapeutic apheresis or immunosuppression (assessed during evaluation).
Realistic expectations and a clear understanding that outcomes vary.
Commitment to close monitoring and ongoing diabetes management alongside and following the programme.
Very young children may not be suitable candidates. Candidacy for this age group is assessed on an individual basis with particular caution.
Potential Benefits of the Combination Therapy Programme
Based on current clinical research and the outcomes reported by patients who have undergone similar programmes, the combination approach may offer:
Reduction in daily insulin requirements: Some patients experience a meaningful decrease in insulin dose, reflecting improved endogenous insulin production.
Improved glycaemic stability: Smoother blood glucose profiles with less variability, reduced hypoglycaemic episodes, and better HbA1c.
Preservation of residual beta cell function: C-peptide levels may stabilise or improve, indicating that surviving beta cells are producing more insulin.
Slowing of autoimmune progression: Reduction in autoantibody titres following apheresis, with the immune rebalancing effect of MSC therapy potentially reducing the rate at which remaining beta cells are destroyed.
Improved hypoglycaemia awareness: Some patients report a reduction in severe or unanticipated hypoglycaemic episodes following treatment.
Improved quality of life: Reduced disease management burden and greater confidence in day-to-day blood glucose control.
Partial remission: Some patients have reported periods of significantly reduced insulin dependency following combination therapy, though this is not universal, and the duration varies.
Outcomes depend on individual patient factors. Research published in peer-reviewed medical journals has reported encouraging findings on the potential role of stem cell therapy and immunomodulatory approaches in Type 1 diabetes. The field continues to evolve.
Potential Side Effects and Risks
As with any medical programme involving multiple interventions, there are potential side effects and risks. These are discussed in detail during your personalised consultation and assessment.
Therapeutic apheresis, common side effects (typically mild and temporary):
Fatigue following sessions
Mild hypotension (low blood pressure) during the procedure; managed by the clinical team
Temporary reduction in clotting factors or immunoglobulins; monitored and managed as part of the protocol
Mild bruising or discomfort at the vascular access site
MSC therapy, common side effects:
Temporary fatigue or mild fever in the 24-48 hours following infusion
Mild headache or flu-like symptoms
Rare: allergic-type reactions; screened for during the pre-treatment assessment
Immunosuppression, risks vary by agent and duration:
Increased susceptibility to infection during the immunosuppression period; patients receive clear guidance on monitoring and when to seek help
Potential effects on renal function, liver function, or blood counts, depending on the agent used, are monitored throughout
Drug-specific side effects are discussed during the treatment planning consultation
Serious complications are uncommon when the programme is conducted under qualified physician supervision with appropriate patient selection and monitoring. All patients undergo comprehensive pre-treatment screening.
Post-treatment guidance: Following treatment, patients receive structured written instructions that include activity recommendations, guidance on ongoing diabetes management and monitoring, warning signs requiring prompt medical attention, and lifestyle strategies designed to support long-term metabolic health.
Why Choose GS Medical Services for Type 1 Diabetes Treatment?
Coordinating access to a multi-component treatment programme abroad is not straightforward, particularly for a condition that requires close metabolic monitoring throughout. GS Medical Services exists to manage that complexity. Our approach is built around the following principles:
Coordinated Access to German Clinical Expertise: We refer patients to clinics in Germany operating within a strict regulatory framework for cellular and apheresis therapies. Treatment is physician-supervised and individually evaluated before any protocol is initiated.
Honest Assessment Before Anything Else: We do not accept every enquiry as a referral. If the evaluation indicates that combination therapy is unlikely to benefit a patient, we say so clearly. Patients deserve that.
End-to-End Coordination: From the first consultation through to long-term follow-up, we manage the process. Appointment scheduling, documentation, medical record collation, travel logistics, accommodation guidance, and telemedicine follow-up are all part of what we do.
Metabolic Monitoring Integration: We work with patients' existing diabetes care teams to ensure that the intensified monitoring required during and after the programme is planned and supported, whether in Germany or back home.
No Hidden Costs: All pricing is provided transparently following the medical evaluation. There are no surprise charges.
Continuity Beyond the Programme: The relationship with the treating medical team does not end when you leave Germany. Structured remote follow-up, coordination of autoantibody retesting, and ongoing clinical guidance are built into the process
Request a Personalised Evaluation for Stem Cell Therapy and Therapeutic Apheresis for Type 1 Diabetes
If you have Type 1 diabetes and are exploring whether combination therapy may be an option for you, the first step is a comprehensive medical evaluation. You may consult Dr. Med. Gerhard Siebenhüner for an expert assessment and personalised guidance.
Your initial consultation will include:
Confidential review of your medical records, autoantibody status, C-peptide levels, and diabetes management history
Honest assessment of whether you are a suitable candidate for the combination programme
Realistic discussion of potential benefits, risks, and expected outcomes specific to your case
Clear explanation of the treatment sequence, timeline, and what the programme involves in practice
Transparent pricing information with no hidden costs
Opportunity to ask questions and discuss any concerns
There is no obligation to proceed following your consultation. Our aim is to give you the information you need to make an informed decision.
Frequently Asked Questions
What makes the combination programme different from standard treatment for Type 1 diabetes? Standard treatment replaces insulin but does not address the autoimmune process destroying beta cells. This programme attempts to address the disease at its source: removing autoantibodies through apheresis, rebalancing the immune system using MSC therapy, and protecting the results with immunosuppression. It is not a substitute for insulin therapy, but it aims to reduce the autoimmune load and support whatever beta cell function remains.
Do I need to have residual beta cell function to be considered? Residual beta cell function is an important factor in candidacy. Patients with some measurable C-peptide have more to gain from the regenerative component of therapy.
Will I still need insulin after Type 1 Diabetes treatment? Most patients continue to require insulin after the programme. The aim is not necessarily to eliminate insulin dependency completely, though some patients do experience significant reductions in requirements. Realistic outcomes are discussed in detail during your consultation.
Is the programme suitable for children with Type 1 diabetes? Paediatric patients require careful individual assessment. Younger children may not be suitable. If you are enquiring on behalf of a child, this will be addressed specifically during the evaluation.
How much does the programme cost? Costs vary depending on the individual protocol, the number of apheresis sessions, and the overall programme length. Transparent, detailed pricing is provided following your medical assessment. All costs, including the evaluation, treatment components, and follow-up, are specified in advance.
How is this therapy regulated in Germany? Stem cell therapies and therapeutic apheresis in Germany are subject to strict national regulatory standards. Treatment is conducted in licensed clinical facilities under the supervision of a qualified physician following an individual medical evaluation. GS Medical Services coordinates referrals to clinics operating within this framework.
Medical Disclaimer
The information provided on this page is for educational and informational purposes only and does not constitute medical advice. Stem cell therapy and therapeutic apheresis outcomes vary considerably between individuals, and treatment may not be suitable for everyone. Type 1 diabetes requires ongoing medical management. Always consult a qualified medical professional before making decisions about your health.